![HR Logo [Recovered]_Full Color Vertical-1](https://blog.healthyroster.com/hs-fs/hubfs/HR%20Logo%20%5BRecovered%5D_Full%20Color%20Vertical-1.png?width=199&height=178&name=HR%20Logo%20%5BRecovered%5D_Full%20Color%20Vertical-1.png)

It’s hard to believe that February is almost over. It seems like just yesterday we were reviewing winter safety tips, and now schools are gearing up for the spring season! But before we trade in the hockey skates and wrestling mats for tennis rackets and lacrosse sticks, we thought we’d take a moment to think about American Heart Month.
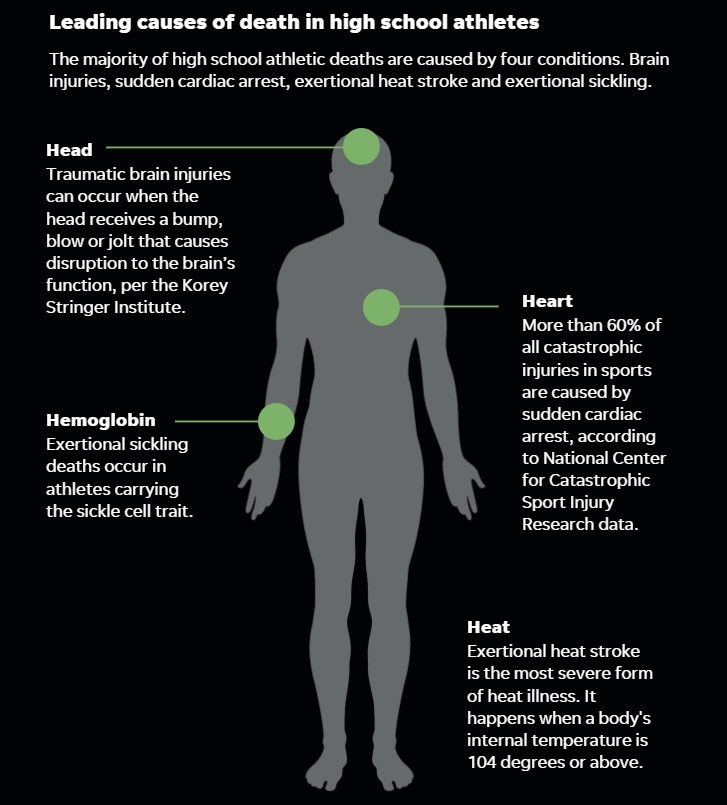
One of the most serious cardiac issues facing athletes today is Sudden Cardiac Arrest (SCA). Though SCA technically has its own awareness month, it’s never a bad time to review the warning signs and prevention measures — after all, being properly prepared just might save a life.
A little background
SCA is a condition in which the heart “suddenly and unexpectedly stops beating.” When this happens, blood flow to the brain and other vital organs stops, which can lead to unconsciousness, permanent brain damage, and death all within a matter of minutes. Almost 300,000 sudden cardiac arrests occur outside of hospitals in the U.S. each year, including the 2,000 patients under the age of 25 who die of SCA annually.
It’s important to understand that SCA is not a heart attack. A heart attack, or a myocardial infarction (MI), occurs when blockage within a blood vessel prevents oxygen from reaching the heart tissue. SCA, on the other hand, is a cessation of the heart’s pumping caused by arrhythmia, an irregular heartbeat prompted by issues within the heart’s electrical system. While some MIs can additionally cause cardiac arrest, there are numerous other conditions that can trigger an SCA-inducing arrhythmia.
Because intense physical activity is one of the stresses that can cause the heart’s electrical system to fail, SCA is a serious concern for athletes. (In fact, one of the first reported cases was Pheidippides, the Greek soldier who collapsed after running 24 miles from Marathon to Athens to announce victory over the Persians.) Another common cause is Commotio Cordis. Caused by a “blunt, non-penetrating blow to the chest,” Commotio Cordis accounts for 20 percent of sudden cardiac deaths in young athletes.
While athletes with underlying heart issues are at a higher risk, as many as 80 percent are asymptomatic until SCA occurs, and some causes won’t be detected through pre-participation screening. Furthermore, SCA can occur in athletes who exhibit no risk factors and appear otherwise healthy. It’s thus imperative that athletic trainers understand how to recognize and react to SCA as quickly as possible.
Signs and symptoms
Just one in 10 students who suffer SCA survive, but survival rates improve drastically when proper steps are taken within three to five minutes of collapse. In fact, the greatest factor affecting survival is the time from arrest to defibrillation. If an athletic trainer can recognize the symptoms of SCA within a quick window, they can optimize the chances of saving the athlete’s life.
While any unexpected collapse should warrant consideration of SCA, additional symptoms in male athletes include chest, ear, or neck pain; severe headache; excessive breathlessness; vague discomfort; dizziness and palpitations; abnormal fatigue; and indigestion or heartburn. In female athletes, symptoms include center chest pain that comes and goes; lightheadedness; shortness of breath; pressure, squeezing or fullness; nausea or vomiting; cold sweats; and pain or discomfort in the arms, neck, back jaw, or stomach. Additionally, seizure-like activity occurs in half of young athletes with SCA, so seizures should be perceived as SCA until proven otherwise.
Prevention and preparedness
All athletes should undergo cardiovascular screenings before participating in competitive sports. This should, at minimum, include a comprehensive review of medical and family histories, as well as a physical exam. If possible, an electrocardiogram (ECG) should also be used to identify underlying heart issues that may put an athlete at risk for arrhythmia.
However, as we mentioned above, SCA can occur in athletes who exhibit no risk factors, so it’s essential that schools, clubs, and sports facilities develop an emergency action plan to respond immediately to suspected SCA. This should include recognition of SCA (see above), calling 9-1-1, initiating early CPR beginning with chest compressions, using an AED (see below), and transporting the athlete to a hospital capable of advanced cardiac care. Remember that once the heart stops beating, death is imminent within minutes, so the emergency plan should be activated as soon as possible. It should incorporate an effective communication system, ensure that first responders are trained in CPR and AED use, and be coordinated with the local EMS agency.
AEDs
Perhaps the most important aspect of a facility’s emergency action plan is its access to an automatic external defibrillator (AED). Studies have shown that the survival rate from SCA drops 10 percent for every minute that passes without defibrillation, and in cases where CPR is provided and defibrillation occurs within three to five minutes, survival rates have been reported as high as 74 percent. It’s therefore recommended that all facilities have an AED on-site and readily available within three minutes, though one minute is ideal. Additionally, all athletic trainers, medical professionals, coaches, parents, and athletes should be educated annually on their location and use so that an AED shock can be administered swiftly and properly in the event of SCA.
Have a great final week of American Heart Month!